|
| A nurse checks a patient's intravenous drip at Xincheng Community Health Center in the city of Huangshan, Anhui, on Aug 31. A full-scale reform of grassroots health services was rolled out across the province on Sept 1 following a pilot program that started in the spring of last year in 32 counties. |
 |
| Zhang Gongyong has been the only doctor in the impoverished Qianshan village since 1974. He is one of many village medics who will be affected by the rural medical reform in Anhui, with his annual income expected to fall by 5,000 yuan this year. |
 |
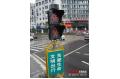
| A pharmacy worker dispenses medicine to a man at the Xincheng Community Health Center on Aug 31. As the patient lives in a pilot zone for the rural medical reforms, he received a 10 percent discount on the price of the drugs. |
Reform a boon for patients, gloom for clinics. Hu Yinan reports from Anhui.
When farmer Wang Shunde visited his village medical clinic in eastern Anhui province with a stomachache, his doctor diagnosed him with acute enteritis, gave him an infusion and prescribed four drugs.
Ordinarily, the bill given to the 56-year-old as he left the clinic on Aug 31 would have made him feel worse than the swollen intestines he arrived with. However, as a resident of the impoverished Qianshan village in Shexian county, a pilot zone for rural medical reforms, he received a 10-percent discount on the drugs.
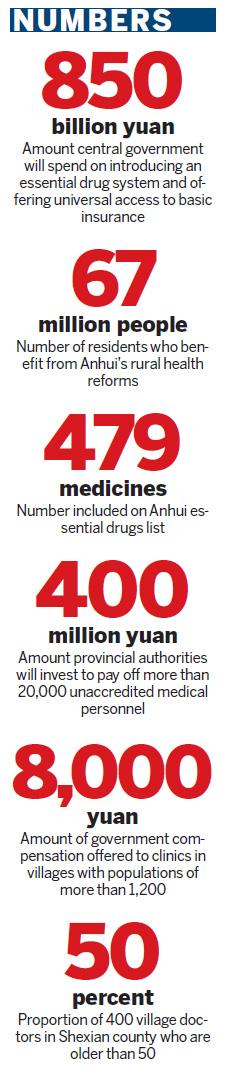
One day later, the price-cutting initiative was rolled out across the province, allowing 57 million people to benefit from efforts to radically restructure the profit-driven township and village medical institutions, the backbone of China's three-tiered healthcare system.
Anhui is the first province to start a full-scale reform of its grassroots health network since the spring of last year, when the central government unveiled plans to spend 850 billion yuan ($125 billion) to introduce an essential drug system and offer universal access to basic insurance.
"The purpose of the initiative is to abolish the existing system, which relies on health providers selling drugs to fill their financing gap," said Gao Kaiyan, director of Anhui's health bureau and the mastermind behind the reform. "It's the first such experiment in our country."
Following the collapse of community-funded healthcare for farmers in the early 1980s, market-oriented reforms helped privatize the sector.
Government spending fell from 36 percent of the total health expenditure in 1980 to 15 percent in 2002, according to figures from the Ministry of Health.
While government budgets for health institutions diminished, the liberalization of the pharmaceutical market drove up the prices of medicine considerably. Hospitals were able to sell drugs at a 20- to 30-percent markup over wholesale costs.
As a result, the amount being shouldered by individual patients soared from 21 percent in 1980 to 59 percent in 2000. In Anhui, the average inpatient charge in township health centers rose 251 percent between 2005 and 2009.
"For a long time now, 60 to 70 percent of grassroots health institutions run on the profits they make from medicine prescriptions," said Gao. "The more a physician prescribes, the higher their revenue. This results in irrational drug use, over-prescription of antibiotics, the corruption of health workers and high drug prices."
An industry veteran of almost three decades, Gao says his comprehensive reform is necessary to "break the system".
Since Jan 1 this year, Anhui has launched a series of bold measures involving 4,811 health clinics in 32 pilot counties, affecting more than 20 million people. The reform includes reinstalling a public-purpose grassroots health system by thoroughly reshuffling existing mechanisms to deal with administration, personnel, income distribution and pay.
The move has brought township and village clinics back under the umbrella of county health bureaus, which, together with finance and labor authorities, are responsible for approving personnel quotas, fixing budgets and evaluating work.
Rather than being offered permanent employment (a core component of the cooperative medical system under the planned economy), grassroots health workers in Anhui are now contracted to avoid egalitarian practice and encourage good performance.
Provincial authorities have also taken control of the bidding for, buying, supplying and distributing of all 479 medicines on the compiled essential drugs list (it has 172 more drugs than the State formulary of basic health insurance), which was previously handled by physicians in towns and villages.
The measures helped cut the prices by about 50 percent in the pilot sites during the first half of this year, according to Anhui's health bureau.
Gao hailed the reform as "orderly, powerful and efficient" in regulating drug costs, combating irrational drug use and streamlining the personnel structure of grassroots health providers.
Money injection
To continue the reform, the province will need to spend roughly 1.7 billion yuan a year. The vast majority will go to township health centers, while the rest will be spent in village clinics run by 67,000 rural doctors. However, significant challenges remain and as Gao puts it: "Any reform is a radical adjustment of interests our greatest problem is the people problem. Local officials historically governed township health clinics in Anhui and their relatives too often occupied a majority of posts there.
"Our investigations found that although many of these clinics had 20 to 30 staffers, they relied on just three to four people who actually worked," he said. "The others were illiterate or barely finished elementary school. No sustainable development can be achieved without abolishing this personnel system."
Even after failing to obtain the proper accreditation, the sheer number of redundant staff, particularly in poor and remote counties, suggests they cannot simply be let go.
For example, half of the grassroots health staff in Guzhen county were asked to leave their jobs under the pilot initiative - but only 13 actually did so. About 340 workers were instead put on a three-year paid probation period.
In an August report to provincial authorities, county officials argued that the compensation they need to pay for redundancies - an estimated 5.4 percent of the county's 2010 financial revenue - is too great a burden.
To avoid the issue spiraling into a crisis, Anhui authorities will inject 400 million yuan this year to pay off more than 20,000 unaccredited medical personnel, some of whom will receive administrative posts instead of being fired.
"I'm not even going to talk about the money problem the utmost concern is to ensure stability," said Gao. Yet, most of the challenges raised by the reform have to do with money.
Internal half-year self-assessments provided to China Daily show that 13 of the 32 pilot sites listed limited finances as the foremost barrier to further reforms.
Some also complained about the mounting debts of township health clinics due to over-expansion in recent years, an issue that has not been addressed by the reform.
"Grassroots health institutions in the 32 pilot sites carry a debt of more than 400 million yuan. Across Anhui, that figures is about 1.4 billion yuan," said Gao.
"The issue still hasn't been addressed too well but we're looking into it," he said, before stressing that the initiative for the entire province "will be proven effective in half a year".
Fall in patients
Health chiefs in all 32 pilot sites signed responsibility agreements in late June that bind them to "achieving comprehensive reform tasks" by March 31, 2011.
Bi Pumin, director of the city health bureau in Huangshan, said the most important indicator of success is whether or not people in towns and villages get cheaper access to healthcare.
However, this cannot be done quickly, he warned.
"Medical reforms in the 1990s and early 2000s attracted a great deal of money from (patients) and boosted health departments, but officials realized that if we left healthcare solely to the market, the people would suffer," said Bi. "That's why we must rebuild a public-purpose system led by the government. The problem becomes how we can introduce a competition mechanism to motivate workers."
The reform has reduced revenue considerably for a third of Huangshan's township clinics. Overall, the number of outpatients fell more than 60 percent during the first half of this year compared to the same period in 2009, which in turn has led to sharp decreases in the incomes of grassroots physicians.
Although township clinics have been stopped from profiting from drug sales, government subsidies have not yet caught up in many areas, posing a dilemma for managers.
Xincheng Community Health Center, Huangshan's highest-rated rural clinic in terms of performance, made 800,000 yuan in 2009 but has witnessed a dramatic decline in revenue following the reform.
Striking a balance between covering costs and providing public services is a challenge, said its director, Cheng Libin.
"With minimal subsidies, we're still pretty much on our own with operating costs," said the 37-year-old. "We can probably earn 400,000 yuan this year, provided each of our 30 or so staffers brings in about 15,000 yuan in revenue.
"Any more would be a stretch, unless we're determined to make profits again. There's still room for profit," he added, referring to the unnecessary infusions ordered by doctors looking to make extra money.
On average, about six out of 10 inpatients at rural clinics are given infusions, according to Ye Lianggui, Xincheng's deputy health director. His bureau has ordered all clinics to cut inpatient infusion rates by 70 percent this year.
Even Cheng's center still gives infusions to half of its patients, however.
"It's a conflict," said the health center boss. "If they want us to meet the revenue requirements, this is how we're going to do it. We would've been much better off had these missions not been assigned but that would be a great financial burden on the government."
In response, Ye acknowledged infusion rates are difficult to contain under the circumstances but insisted the reform is on the right track.
"If we just let it go and allow them to make profit, the tasks of grassroots health workers would've been extremely simple: Just go catch patients and butcher them," he added. "Without this reform, medical costs would only go up year after year."
Doctors' fears
In rural areas, problems generated by previous market-driven reforms are causing fresh headaches as officials try to restructure village clinics into public health facilities.
Under the new initiative, provincial health authorities pay annual compensation of 8,000 yuan to each clinic in a village with a population of more than 1,200.
However, 17 of the 32 pilot sites said in their assessment that the earnings of rural doctors had gone down exponentially and needed immediate intervention.
Dongzhi, one of the pilot counties, reported that its doctors on average made 20,000 yuan a year before the reform - 70 to 80 percent coming from drug profits. The regulation of drug prices will cut estimated incomes this year to just 35 percent of that, according to the submitted assessment.
Zhang Gongyong has been the only doctor in the mountainous Qianshan village since 1974 but is not qualified to receive the 8,000 yuan compensation as he serves only 400 people.
The 56-year-old made 8,000 yuan at his clinic in 2009, as well as 2,000 yuan from growing tea and oranges and 1,200 yuan from government subsidies. However, the latest drug pricing regulations mean his total net income will fall by 5,000 yuan this year.
For the time being, Zhang is fine with the changes. "If other people can survive, so can I. Somebody's going to have to work for public health in villages," he said.
Rural youngsters have become much less motivated to join village clinics in recent years and more than half of the 400 village doctors in Shexian county are older than 50.
"Fewer kids are studying medicine," said the veteran medic. "People can make at least 30 to 40 yuan a day as migrant workers. That's not the pay you can expect as a village doctor."
He added: "I'll be here until I'm too old for it. There's no retirement."